MRI reveals the reasons for the noise at the vusi. The current principle of diagnostics and treatment of patients with chronic uterine otitis media Treatment of sigmoid sinus thrombosis
One day order with a stove є another 1-2 turn-overs. By world
The development of a nipple-like outgrowth in a new one is a new growing cell.
An old-fashioned figure appears at the old man in the stove's bag
ale glibshe, and according to the worn out to the drum empty - lower.
Peches step by step go down and move medially, back and down, pl
A piece of luska to be admired.
Have children early vik enter to the queens (Aditus ad antrum) wide. Z zim
not often tied overnight
st_y of the shell of the drum empty and the queens (otoanthritis).
Nipple-like sprout to establish itself in case of zlitty nipple-like surfaces
Kam'yanistic and lusky parts of the curtain brush. Osvita air carrier
They should be repaired in 4-5 months and it will be enough to finish up to 3-5 years.
Variety of pneumatization and the value of alternating intervals in values
the boiler world to lie down from the vika, the zagalny development of the child, from the aeration polo
stey of the middle wuh, having transferred the fiery illnesses.
Zapalenya middle vuha and zagalny dystrophia lead to the formation of children
types of pneumatization of the nipple-like outgrowth,
For a small part to cover the process of pneumatization.
Pererakhovani factors are injected on the bud of mastoid growths. once
razr_znyayut pneumatic, diploetic, sclerotic tipi.
I am very aware of the fact that in the English period of hearing it is
b in the middle of the ear, a slimy shell is introduced, which is whistled in and with about to i m ku
bicheskim epitelієm. Until the end of the 1st rock tsia slizova shell of re-enactment
To be in the current mucous - per and the rest of the coffin. PROCESSING PROCESSING PROCESSING
The membrane of the mucous membrane is tightly bandaged during the process of pneumatosis
tsії. Already in embr і about n a l n o m period n a h і n a є t s I і n in a g і n and c і I z l і s і s t o ї
shells from empty drum in the cave and from her in the nipple-like
an outgrowth. As a result, an outgrowth is formed with normal pneumatic
what type of budovi.
The process of pneumatisation of the nipple-like extension takes one hour
Itself with the substitutions of the diplomatic cist fabric and compact, like in
the main one ends at the 8-12 rocky days and starts with a new development
systems and pneumatization of the nipple-like outgrowth (Fig. 2.7).
The process of pneumatization is not only built up to the slime
shells from the side of the liver. 3-5-month period for the development of the pers
a prominent outgrowth is repaired in the active traction of the sternocleidomastoid
stsevidny m'yazi, how to zbіlshuvatisya in a whole lot and width is good
donate robots, so come to the call vertical encampment tuluba i
by turning the head.
The process of pneumatization of the nipple-like protuberances from both sides does not depend on
somewhere overnight. Tse slid vrahovuvati at assessment of roentgenograms at
at the Antrum.
BABY Otorhinolaryngology
Small. 2.7. Type of nipple-like appendage.
a - diploetic; b- sclerotic; c - pneumatic.
Slide the nipple-like appendage and cyst part of the ear canal
child until the end of the styloid opening and the top
one nipple-like appendage; see him, call him sleepy and yar
with n and m openings in the postnatal period, but not the same change.
Above the opening of the styloid opening into the connection from the outside
The nipple-like outgrowth grows with injuries of the facial nerve during anthrotomy.
To the inner stage of the nipple-like outgrowth of the lagoon sigmoid sinus (sinus
sigmoideus). The newly born wines do not have a swollen cyst bed and do not
pass in the middle into the jugular vein with a straight cut; cibulin yarem
noi veni (Bulbus venae jugularis) it is only until the 9th month of the year.
Topographic and anatomical peculiarity of the sigmoid sinus tightly tied
with the development of the nipple-like outgrowth.
The pecher is located at the end of the sign of the sine
foot baby - 5.9 mm)
children 1-3 rock and up to 4.2 mm in 4-7 rock. At the connection with such a view
Chicken thrombosis of the sigmoid sinus in children of early age
Nіzh at grown-ups, and accelerated to have the character of septicemia.
Practical value of sinus saline glybin. Do roku won zi
set 2.4 mm, from 1 to 3 rocks - 3.2 mm, from 4 to 7 rocks - 4.5 mm. As a result
redistribution of the sigmoid sinus in childish is estimated to be approximately
3% of vipadc_v, which goes to vrahovuvati during surgical engagement.
From the furrow of the sigmoid sinus to the lower part of the chi canal
of the fore nerve to become 5-10 mm.
Placement between the styloid opening and the top of the nipple-like
There is little outgrowth in an early child's whit (up to 7 mm). tse slid
wrahowuwati at conducted research projects and anthrotomies.
facial nerve (P. Facialis) until the moment of the people, it is already laid in a kistkovy ka
Got_vka and maє the same diameter as in grown-ups.
In children, there are drops in the tympanic canal of the facial nerve in children up to
4 rokiv nemaє kistkovoi stinki, scho spriy swift development of the paresis of the face
| |
sick wuh
nerve with gostrich otitis media. If you have a vipad, the cistkova wall is even thinner,
the maximum thickness is 1 mm, approx. 20%
cents. In the wake of the price, the lines grow overgrown.
The children of the first rocks of life have been replaced by the channel of the Lyceum
nerve i spina suprameatum.
The external opening to the canal of the facial nerve grows larger than the horizon
tally, lower in the elderly, and lie on the surface. Zvyazu z zim facial paresis
For a quote: Garove Є.V., Garove E.E. The current principle of diagnostics and treatment of patients with chronic gross otitis media // RMZ. 2012. No. 27. S. 1355
Chronic gnarial otitis media (CHSO), thanks to the data of the WHO, is an important problem of protecting health, which is not economically and socially significant. HGSO is the main reason for dullness. For the purpose of the VOOZ, KhGSO, there is a chronic infection of the middle whale and drum overflow, which is supervised by otorrhea of more than 2 types. ...
In all the svitі of the KhGSO suffer from 1 to 46% of the individuals who live in the developed regions, which are developing. The price is about 65-330 million, 60% of them may mean less hearing. The expansion of the KhGSO in our land is from 8.4 to 39.2 per 1000 population. A number of patients with ENT pathology, who need additional help in ENT hospitals, 5.7-7% suffer from HGSO. The breadth of HGSO with cholesteatoma in the population is 0.01%. The peak of the people falls in the middle and third decade of life. Cholesteatoma occurs in 24-63% of patients with chronic hepatitis C in case of localization of drum perforation. Cystkova resorption in otitis with cholesteatoma occurs in 78.8% of cases. The very same HGCO with frequent sharpened є the reason for otogenic acceleration.
The transition from the state of the middle otitis to the chronic mating with inadequate treatment of the state of the disease (the sign of antibiotics, nonspecific for the flora, which has become ill). Chastі epіzodi GOSTR serednogo otitis scho prizvodyat to torn down fіbroznogo ball barabannoї peretinki, anatomіchnі osoblivostі Budova serednogo Vuh (vuzkі expanse barabannoї porozhnini, adіtusa, kishenі zovnіshnogo attic, sinusitis gіpotіmpanum i retrotіmpanalnih vіddіlіv) spriyayut trivalim latent Ignition Process, SSMSC, zakіnchuyuchis rozvitkom fіbroznih Change log , you yourself will be able to interrupt the process. Disruption of the mechanisms of the muscular immune system, chronic pathology of the nasopharynx and the emptying of the nose to produce a stiff negative clutch in the empty drum, retro-empanic space, cells of the nasopharyngeal secretary process and up to the trivial guest
For the classification І.І. Potapov (1959), based on the size, localization of the perforation of the drum overturning and the options for overcoming the disease, seeing mesotympanitis, epitampanitis, epimesotimpanit. I will look at those who are more significant, develop the formation of mucositis, the development of fibrous-cystic, tympanic-sclerotic, carious and cholesteatomical processes in the middle of the In the case of a specific approach to a look, a classification is given to the need for a glance.
Mesotympanitis (chronic tubotimpalny middle otitis media, H 66.1) is a form of HGSO with localization of perforation in a stretched form of a drum-like cross-flow, with an apparently friendly prognosis; Protest of the middle of the intraoperative sorcerers, there are signs of changes in the auditory handles (the spine of the cowadl, the structures of the stirrups, the handle of the hammer) as a legacy of the transferred sharpening process. Earlier, it was important that the cholesteatom process was not typical for mesompanitis, however, at the end of the day, the cholesteatoma of the mesompanum appears at the end of the day, and the cholesteatoma of the mesompanum appears in the last few days. According to the statistics of the microsurgery of the MNPTSO for the period from 2009 to 2012, in 12.4% of cases in the middle of the operated patients with the diagnosis of "mesotympanitis", the cholesteampanoma of the meso was detected.
Epitympanitis (chronic epitimpanic-antral otitis media, H 66.2) is a form of HGSO, which is characterized by localization of perforation in a loose type of drum overflow. Often, gliboki retraction colonies are formed from the destruction of the lateral attic, epidermoisation of the attic and retrompanal appendages, by means of cholesteatomy. The cholesteatoma is a chronic ignition process, which is characterized by progressive growth and destruction of the epithelial and cyst structures of the middle air. With this form, the destructive process is promoted to the attic, aditus, antrum and cells of the nipple-like sprout, not too often from the invading epidermis in the structure and ruining of the keys of the anatomical structures , promontory wall). For danimy doslіdzhen, nіzh less defect in the unstretched view of the cross-flow, more and more obsyag ruinuvan in the empty drum and antromastoid view. Due to the localization process (the upper surface of the drum emptying), the self-cleaning of these types of waste is difficult during To that, when diagnosing this form of illness, early sanitary surgery is shown.
In case of epimesotism, signs of both forms are observed.
Morphologically, the cholesteatoma of the middle air is characterized by proliferation of epithelial cells and the formation of granulation tissue. It is very important to allow for the links between the developmental cholesteatomy and the callous auditory passage on the basis of the established identity of the expression of the epithelial markers of the cholesteatomy and the epidermis of the external auditory passage.
I see a kind of a cholesteatomy. In the given statistics, only the options are displayed. On the current day, there are 5 theories of the pathogenesis of nabutoy cholesteatomy.
1. Migratsiyna theory, which means that the growth of squamous food into the empty middle woh through the perforation of the drum mash.
2. According to the theory of the retraction colon, the cholesteatoma develops from the retraction colon, which is accepted as a result of chronic dysfunction of the auditory tube and is not built up to self-purification.
3. For the theory of hyperplasia of the basal cells of the cholesteatoma, it is pretended to be the path of invasive papillary growth of keratinocytes in the main ball.
4. According to the theory of metaplasia, there is a metaplastic transformation of the epithelium of the mucous membrane of the middle air into the cholesteatomic matrix.
5. In the last 10 years, another theory of the development of cholesteatomy appeared: the theory of retraction and proliferation, which is the basis of the theory of invagination and the theory of basal cells. The proliferation of the epithelial cells of the retraction colon changes under the inflow of the ignition stimulus of the subepithelial ball, which leads to the formation of cholesteatomy.
There is also one of the mechanisms of development of cholesteatomy behind an intact drum-like overflow and coverage of microcholesteat for infection of epithelial cells through the development of the main membrane in the subepithelial tissue of the secondary tissue.
Unimportant for a great number of dosages held in the development of rock and direct to the development of cholesteatomy and the reasons for the development of cholesteatomy, one mechanism for better cholesteatomy options is not clear. However, there is an anatomical change in the formulation of cholesteatomy, however, for more and more options. Until the 4th date, the mechanical block of the tympanic diaphragm, the blockade of the aditus, the posterior tympanic sinus and the dysfunction of the auditory tube are affected, to create a stiff vacuum in the anthromastoid retinal space, which changes the brain space behind the hollow space. Retraction of the cross-flow is formed anteriorly and posteriorly to the head of the malleus, leading to the formation of cholesteatomy in the anterior attic and supratubar sinus and in the intestines of the late attic (the Prussians' intestines, the Kretchman's intestines, the Troelch's swarms). Retraction of the cross-flow in the anterior and posterior sides of the stretched part of the drum cross-flow can cause the dzherel to develop cholesteatomy in the mesothimpanum. In the supratubar sinus, in 50% of cases, keratinization of the epithelium and transformation of it into a cholesteatoma are repaired. 60% of patients have a friendly muscle for the development of cholesteatomy є subphase and posterior sinuses (sinuses are not visible in the anterior area).
On this day, there are also no single thoughts about the causes of recurrence and aggressive development of cholesteatomy. Aggressive behavior to the matrix of cholesteatomy, newer, is summarized in the development of lytic enzymes, lymphokines, cytokines and factors in the growth of new cells during the ignition process. In numerical pre-slugs, a deterioration of proliferation, differentiation and migration of keratinocytes in the cholesteatom matrix and the order of activation of perimatric fibroblasts was demonstrated. The whole process is going along the path of accumulating and ruining the clan sided conversations (debris) on the epithelial side of the squamous epithelium, which has invaded the vastness of the middle world. Aggressive with a stretch of cholesteatomy, a lot of pre-aggressors, it can also tie with pathological flora, invariably supervise the KhGSO.
As a rule, in patients with HGSO and cholesteatoma, there is a change in polymorphic (aerobic-anaerobic) flora, it is easy to develop from 2-3 microorganisms. Aerobic flora is a chronic ignition process in 60.3%, anaerobic - in 38.2% of cases. The main microorganisms, which infect cholesteatoma, Pseudomonas aeruginosa, are isolated in 31.1% of vipads, Staphylococcus aureus - in 19.1%. Coagulase-negative staphylococcus appears in bagatioids.
Anaerobic coca hangs in the middle of anaerobic coca: Peptococcus and Peptostreptococcus (in 17.2% of cases), and more - Bacteroides (in 12.4%). Anaerobi, schooled in isolation, more often to develop important accelerated HGSO (mastoiditis, internal scalp acceleration); 1.4% attack on the fungal flora (often Aspergillus).
The antibiotic resistance of this flora is a great problem. One of the reasons for this is not only polymorphism, but rather building up to the formation of biofuel on the surface of the squamous food. Bioplates are the production of microorganisms, which are placed in the moisture to produce the matrix and naturally adhere / grown on the surface of the tissue. With HGSO, especially with cholesteatoma, a change in polymorphic bioplasty is formed, which reveals the colonies of aerobes and anaerobes. Microcolonies of bacteria can be stored in an acelyular polymeric matrix, in the warehouse of biofuels they can be formed into cholesteatom by the matrix. In connection with the cym of acceleration їх standard parkan for microbiological dosage, the stench grows non-irritating for antibacterial (systemic and topical) therapy in standard dosages. To that ailment, it is constantly given to re- and superinfіcіrovanie, and only surgical treatment by the same method of therapy. One of the versions of the causes of recurrent cholesteatomal process in the middle is the formation of strong bioplastics to the combined surgical and conservative antibacterial treatment.
Bacteria in the middle of biofilms actively metabolize and produce endotoxins and other life-giving products, before starting a classic way of ignition processes and sprites to a faint ignition process. There is also a stench you can put in without a signaling system epithelial cells (for the adhesion on the surface of keratinocytes, for example, P. aeruginosa), as a starting point for differentiation and proliferation processes. Dani mechanics injected into his heart lead to aggressive cholesteatom matrix and cystic resorption.
Diagnostics of HGSO is guilty of including, except for the collection of scarg and anamnesis, a retinal examination of ENT organs, including otomycroscopy (otoendoscopy), endoscopy of the emptying of the nose and nasopharynx. When analyzing scarg and anamnesis of illness, I respect the triviality of the illness, the frequency of the aggravation of the process, the nature of the vision from the air, the manifestation of vestibular damage and the presence of early entry from the HGSO. When oto (endo-) microscopy, it is necessary to clarify the localization and growth of retraction intestines, perforation, defect (calcification, epidermisization, and tucking of the bone margins), destruction, the nature of the vision (yaksho є) in the drum emptying (slime, gniyne, signs of fungal infection). If it is necessary, then take a video collection for a further microbiological preliminarily sensitiveness of flora to antibacterial drugs. Therefore, it is necessary to establish the standard of functions of the hearing tube, steps of passage. Dal to carry out tuning fork and audiologicheskihne to assess the hearing (the appearance of the neurosensory component, the value of the cysto-periodic interval, the hearing of the contralateral sound).
If you are susceptible to cholesteatomic process in the middle stage, it is necessary to carry out an X-ray of the early stage cysts. Bagato information about the structures of the skroevoy brush can be trimmed with the vicorian high-resolution computer tomography(CT) with a crochet of 1-2 mm in axial and coronary projections, viconious in the stage of remission. dane doslіdzhennya dozvolyaє viznachiti nayavnіst patologіchnogo substrate in porozhninah serednogo Vuh, zberezhennya lantsyuga auditory kіstochok, anatomіchnі osoblivostі Budova soskopodіbnogo vіdrostka i lay structures (peredlezhannya sigmovidnoї sine nizke Stoyanov bottom serednoї cherepnoї fossa, a temple roztashuvannya Tsybulin yaremnoї Veni) and takozh nayavnіst destruktsії stіnok barabannoї porozhnini, antrum, stun canal of the facial nerve i internal wuh... Unfortunately, due to the nature of the pathological substrate (cholesteatoma, fibrosis, granulation, exudate, gniy, cholesterol granuloma), it does not seem possible to directly control the thickening method, it is possible to deprive him of it by secondary tomography. In the interpretation of CT, an important role is played by the quality of education.
According to CT scan data of ear cysts for mesompanitis, there is a characteristic change of mucous membrane in the drum emptying, scarring process near the lance of the auditory brush, a possible defect in the lance, often for the defect of the lance of the poor devil. Antrum with mesompanitis in the stage of remission becomes pneumatized. I am familiar with the chronic process of sclerosing the clitin of the nipple-like growth. Cholesteatoma in patients from HGSO is most often CT-signs of osteo-destruction and supernatant growth of hearing cells by means of a lancinum, due to the appearance of the contours in the drum empty
Unimportant on the high informativeness of CT scan of rone cysts, diagnostics will start the process in the middle level and the tactics of detecting ailing HGSO lie in a comprehensive assessment of all methods of reading. At the same hour, the CT scan of the skinny cells play a great role in the design of the surgical approach and surgery for the patients from the KhGSO.
In the last few years in the foreign and recent literature, it appeared about the possibility of accurate diagnostics of cholesteatomy in the skinny cyst behind the additional magnetic resonance tomography (MRI) in singing modes.
conservatively
Antibacterial therapy (zagalnaya abo miscev) is indicated in the following types: The tendencies of the rest of the rocky and the emergence of antibiotics in the planned, often "clean" medical interventions. When antibacterial therapy is recognized, it is necessary to provide special flora and sensitivity to antibacterial drugs. Some of the most effective and, apparently, are often recognized antibacterial drugsє fluorochinoloni II generation and respiratory fluorochinoloni (ciprofloxacin and levofloxacin). Vibor preparations are also used for cephalosporin and amoxicilin with clavulanic acid, for the stench in the minor world of active against anaerobic flora.
At the time of the change of flora, a combination of 2-3 preparations for perechrynaya infusion at once on all types of pathogenic microorganisms, for example, cephalosporin, fluoroquinoloni and metronidazole, is stagnant. Combination of topical antibacterial drugs with anti-fungal diseases is possible.
It remained an hour that a lot of foreign authors appeared about the stagnation of principally new antibacterial forms, especially antibiotic-resistant forms (S. aureus, P. aeruginosa) and fungi. So, it is successful to carry out additional testing of ototope antimicrobial peptides on misha.
surgical treatment
Hirurgic tactics in case of different forms of HGSO development. For a cob, it is necessary to take the form of the HGSO and the stage (sharpening abo remіsіya).
At the stage of the sharpening of the operation, it is shown only when the patient's development is risky I will load my life I will become (intracranial accelerated, labyrinthitis, mastoiditis, sigmoid sinus thrombosis, otogenous sepsis), even if heated, stiff to conservative therapy.
With an accelerated relocation of the HGSO, extended sanitizing operations are carried out (the classic expansion of the radical surgery is extended to the dehiscence of the dura mater and the sinus membrane); With a whole stage of surgery in a drum empty, it is necessary to visit the opticians.
In vsіh іnshih vipadkah operatsіya guilty provoditisya routinely in spetsіalіzovanomu vіddіlennі of obov'yazkovim zastosuvannyam mіkroskopa so on the title of "dry vusі" oskіlki tse not tіlki zmenshuє obsyag operatsії, zabezpechuє well vіzualіzatsіyu, zberezhennya nezmіnenih structures, ale i spriyaє reparatsії tkanin pіslya operatsії і changes to the relapse process.
In case of mesompanitis, carry out auditory surgery - tympanoplasty of I, II, III types in the formation of prostheses from the stage of prosthetic repair of hearing cells from the prosthesis of adult prostheses (titanium prostheses of the cartilage and cartilage) In case of epimpanitis, epimesotimpanitis, especially in the presence of cholesteatomy in the first place, sanitation is shown. If it is worthwhile, then hearing improvement is carried out at once. Emptying the middle of the whale of the sick from the back of the ear canal (it’s about the back wall of the ear canal) and the critical technology from the time of the different options for the healthier’s hearing With a wider access, with more opportunity for the surgeon to look around the operation area.
Shown vikoristannya Closed-up techniques sanuyuchih operatsіy at medial otitis nastupnі: obmezheny karіoznoї-granulyatsіyny protses a penthouse-antral oblastі, obmezheny epіtimpanіt, attіkalnaya obmezhena cholesteatoma, cholesteatoma barabannoї porozhnini, pnevmatichny type Budova soskopodіbnogo vіdrostka, Young vіk patsієnta, nastrіy patsієnta on revіzіyu away. Prior to critical options for operations, the operations are carried out for the protection of the most recent attic different options with a small restoration of cikh stinks. During cycles of operations, the visceral matrix of cholesteatomy is visibly increased, the visualization of the visible stems by a fragment of auto-tissue or autocartilage and with elements of tympano- and ossiculoplasty. There are no simple options for supercritical techniques with different surgical approaches using different methods of plastics of distant walls, elements of the lancet of hearing cells and drum mismatch.
Basic tendentsієyu ostannіm hour Je poєdnannya vіdkritoї i zakritoї techniques tobto vikonannya attіkoantro / mastoіdotomіі of oblіteratsієyu antral / mastoіdalnoy vіddіlіv autobone, autohryaschom, m'yazovo-fastsialnі klaptem, m'yazovim klaptem on nіzhtsі abo whether Yakima іnshim bіologіchno іnertnim synthetical materіalom ( " StimulOss ", hydroxyapatite, bіokeramika). As a result, the anatomical structure of the middle and last year is preserved, it is close to the vicious one; emptying operationsі, also, the need for additional caution otosurgeons.
According to the data of the young authors, the functional results (improvement of hearing) do not give rise to certain indications in case of stagnant critical and critical methods, such as the frequency of recurrence of cholesteatomy (at close-ups - 3-13.2%)
All sorts of people have an active discussion about stages surgical treatment ailing HGSO. So, M. Sanna s spivavt. (2003) Vvazhayut, ossiculoplasty, tympanoplasty was carried out, giving better functional results. We will authorize the authorization to see the techniques, we will get some feedback in case of remaining recurrent or residual cholesteatomies. In cases of cholesteatomia, the process also involves stages - sanu and reconstructive stage.
For the sake of access and the type of surgical treatment, the number of stages to be found in the centrality of the surgeon, the position of this surgical school, in the type of surgical treatment, and from the first transition. A number of surgeries vvazayut for brightening only the opening options for operations, carried out by the first entrance, and for closing, carrying out the endaural. It is important to take into account the basic principles of surgery of the HGSO, in such a way as to spare as much as possible the sanitation of the empty middle age with the maximum functional result for the patient, so as to achieve adequate hearing (as well as possible), fast time of the term I will look at the price of a large number of surgical procedures, one-stage surgery.
In case of vikonannyh surgical engaging on a quick brush, it is necessary to maximally vikoristovuvat the entire arsenal of pre-instrument instrumental possession: micro-mirrors, otoendoscopy. It is not a matter of re-evaluation of the endoscope's visor, there are fragments behind a thin (2.7-3 mm) endoscope with 30o, 70o cutoffs. ), which allows you to change the general operation of the operation or change the surgical access to the less traumatic and space. So, with a suspicion of antrum cholesteatoma or revision surgery through an intrameatal access, using an atticotomy behind the aid of an endoscope, it is possible to look at aditus and antrum or to exclude a recurrence of cholesteatomy. Heads of the combination of microscopes and endoscopes during surgery of HGSO, the frequency of recurrence of cholesteatomy is sharply reduced.
revision of surgery
In a few critical techniques є the need for a “second look” operation - revision of the empty middle air in order to prevent a recurrence of cholesteatomy in 8-12 months. writing operations.
The development of the understanding of recurrent (knowledge of vinicle) and residual (excess of cells in the cholesteatomic matrix) cholesteatomy. A recurrence of cholesteatomy can be diagnosed by a sharp perforation of the neotimpanic membrane, periodic visions of the empty drum and progressive dullness in the long-term period.
If there is any scarg on the side of the patient, a relapse of cholesteatomy can be diagnosed until recently after an additional surgical revision. However, in one of the ways (if the patient does not need to carry out a repeated operation), the problem is resolved and the diagnosis can be exchanged. CT scan of the skin cells is not very informative in assessing the stage of surgery, scraps of scar tissue, granulation, plastic auto-material may, however, be similar to cholesteatoma. Vrahovuvati CT danny can only be done in dynamism (the growth of "mature" coverage by holding out the term of caution). However, it is expensive to achieve an expensive method of diagnostics, and not a skin patient can be allowed.
The rest of the hour was typing in the diagnosis of cholesteatoma, including relapses, after the addition of MRI in other regimens (DWT1, T2, EPI DWI, non-EPI DWI). On the cinnamon cholesteatom, there will be a hyper- or medium-intensity signal in the T2 and DWI b-1000 modes.
In case of recurrence of cholesteatomy, surgery can be minimized (visible cholesteatomy in the obolontsy) or expanded right up to carrying out atticoanthromastoidotomy from visible back signs.
Such a rank, complex preoperative maintenance of patients from the KhGSO, retailer preparation and registration during the operation of the ample arsenal of possession, methods of operation, and how it is necessary to take advantage of the efficiency
This statistic presents the results of operations carried out at the microsurgery department from 2009 to 2012: 978 surgical procedures were involved in the HGSO drive, of which 708 operations were performed on the mesotherapy drive and 270 sanitizing operations In all ailments, the operations were performed in a planned manner and during the period of remission.
In patients with mesotympanitis, tympanoplasty of the I type of viconan in 566 (79.9%) cases, type III - in 134 (18.9%), and type IV - in 8 (1.2%). A thin epidermis or a small cystic cholesteatoma in the boundaries of the empty drum in some cases with a partial lysis of the lanceus of the auditory cysts was detected intraoperatively in 87 (12.3%) ailments. The patients underwent revision of the empty drum for visible cholesteatomy and type I tympanoplasty in 56 (9.9%) cases, type III - in 31 (23.1%). Tympanoplasty of the I-IV types was seen from the back of the autochondral half-plates and auto-facets, which were placed on the hammer handle, kovadlo, head of the stirrups, or more roundly. Ossiculoplasty was seen from the cartilage vykorystannyam with the supporting material (spongostan) from the T-shaped prosthesis viglyad, Columelli, "pills".
In patients with CHGSO with cholesteatoma, sanitizing operations according to the closed type of viconan in 206 (76.3%) cases, in 64 cases (23.7%). Also, all the patients at the preoperative stage underwent CT scan of the skinny cysts, the results of which were taken during the planned surgery and the walk. The yield of the intraoperative henchmen and CT-dosage is 91%. Relatively due to the nature and breadth of the pathological process, the damage to the anatomical structures of the middle ear, the level of auditory damage was observed attiko- (19 types, 9.2%), atticoadito- (100 types, 30.5%) 1%), as well as the dissemination of atticoanthromastoidotomy (25 types, 12.2%) with the appearance of cholesteatomy and simultaneous reconstruction of the lateral stage of the attic, aditus and tympanoplasty of the I-IV types (according to the type of osteoarthritis). Our view of the tactics, which are perceived in the form of microsurgery, is a one-time reconstruction with sanitation.
A series of sanitizing surgeries, performed according to an open methodology, was performed 24 with an endaural approach (atticoanthrotomy) and 40 - with an emergency (atticoanthromastoidotomy). The less access, the less the number of empty spaces and the more beautiful functional result: shorter period of time, less reparative surface area, more beautiful hearing function. In case of stagnation of critical techniques, the endaural approach has been shown to obliteration of the antrum, aditus / atticus by autochondral, autobone fragments and by replacing the membrane with the order of tympanoplasty of the III-IV types. In case of vikonanny surgeries by the first step, for the sanitary stages, they simultaneously underwent reconstructive tympanoplasty of III-IV types, mastoidoplasty, meatoconchoplasty autologous tissue (autochondry, autologous bone). In 10 types of hearing polyps, the stage was not carried out through an active ignition process.
Recurrence of cholesteatomy in case of vicious closed technique was diagnosed in 17% of cases, in case of congestive technique in 7%.
In such a rank, the effectiveness of the treatment of patients from the KhGSO lies in the complex preoperative maintenance, retailer preparation and qualified performance of the operations for the victories of the optics. On the vibration of the operating methodology, I infuse the character of the process into the middle weight, technical capabilities and the level of preparation of the process. Perevaga will review the options of sanitizing operations for the ailments of the KhGSO amidst a decrease in the frequency and increase of fire and increase in the quality of life of patients.
literature
1. Prevention of hearing impairment from chronic otitis media. Report of a WHO / CIBA Foundation Workshop, London: 19-21 November 1996.
2. Tos M., Thomsen J., Peitersen E. Proceedings of the Third International Conference on Cholesteatoma and Mastoid Surgery. Amsterdam: Kugler & Gehdini, 1989.
3. Otorhinolaryngology: national research / ed. V.T. Palchun. M .: GEOTAR-Media, 2008.
4. Klinichna anatomy of the wuch: Navchalnyy posibnik / O.V. Stratiev. SPb.: SpetsLit, 2004.S. 30-106.
5. Otorhinolaryngology: Essential for patients. Palchun V.T., Kryukov A.I. M .: Medicine, 2001. Ch. 9-10.
6. Sudhoff H., Tos M. Pathogenesis of attic middle ear cholesteatoma: Clinical and immunohistochemical support for combination of retraction and proliferation theory // Am J Otol. 2000. Vol. 21. P. 782-792.
7. Yamamoto-Fukuda T., Hishikawa Y., Shibata Y., Kobayashi T., Takahashi H., Koji T. Pathogenesis of Middle Ear Cholesteatoma. A new odel of Experimentally Induced Cholesteatoma in Mongolian Gerbils // Am J Pathol. 2010. Vol. 176 (6). R. 2602-2606.
8. Jahnke K. Middle Ear Surgery. Recent Advances and Future Directions. Georg Thieme Verlag, 2004. Chapter 4. P. 73-93.
9. Sudhoff H., Linthicum F. Cholesteatoma behind an intact tympanic membrane - histopathological evidence for a tympanic membrane origin // Otol Neurootol. 2001. Vol. 22. P. 444-446.
10. Ricciardiello F., Cavaliere M., Mesolella M., Iengo M. Notes on the microbiology of cholesteatoma: clinical findings and treatment // Acta Otorhinolaryngol (Ital). 2009. Vol. 29 (4). R. 197-202.
11. Wang E. et al. Otopathogenic Pseudomonas aeruginosa strains as competent biofilm formers // Arch otolaryngol head neck surg. 2005. Vol. 131. P. 983-989.
12. Chole R., Faddis B. Evidence for microbial biofilms in cholesteatomas // Arch otolaryngol head neck surg. 2002. Vol. 128.P. 1129-1133.
13. Zelikovich Y.I. CT scan of an early cyst in the diagnosis of chronic otitis media // Bulletin of otorhinolaryngology. 2004. No. 4. S. 42-46.
14. Imaging of the temporal bone. J. D. Swartz, H. R. Harnsberger. Thieme, New york, 1998. Chapter 3.
15. Lee Y. et al. Di-K19Hc, an antimicrobial peptide as new ototopical agent for treatment of otitis media // Acta Oto-Laryngologica. 2010. Vol. 130. P. 897-903.
16. Sanna M., Sunose H., Mancini F., Russo A., Taibah A. Middle Ear and Mastoid Microsurgery. Georg Thieme Verlag 2003, Chapter 5, 13, 14.
17. Reddy T., Shetty A., Dutt S., Maini S. Transcanal atticoaditotomy and transcortical mastoidectomy for cholesteatoma: the Farrior-Olaizola technique revisited // Ann Otol Rhinol Laryngol. 2001. Vol. 110 (8). R. 739-745.
18. Dornhoffer J. Retrogade mastoidectomy with canal wall reconstruction: a singlestage technique for cholesteatoma removal // Ann Otol Rhinol Laryngol. 2000. Vol.109 (11). R. 1033-1039.
19. Certification on the surgery of the middle school. Pidkhodi, myringoplasty, ossiculoplasty and tympanoplasty ed. A.V. Starokhi. Tomsk, Siberian State Medical University, 2005.Vol. 2.
20. Kosyakov S.Ya. Vibration nutrition of practical otohirurgii. M .: MCFER, 2012.
21. Lee W., Kim S., Moon I., Byeon H. Canal wall reconstruction and mastoid obliteration in canal wall down tympanomastoidectomized patients // Acta otolaryngologica. 2009. Vol. 129. P. 955-961.
22. Kim J., Choi S., Chung J. Clinical results of atticoantrotomy with attic reconstruction or attic obliteration for patients with an attic cholesteatoma // Clinical and Experimental Otorhinolaryngology. 2009. Vol. 2 (1). R. 39-43.
23. Kim M., Choi J. et al. Hearing outcomes according to the types of mastoidectomy: a comparison between CWU and CWD mastoidectomy // Clinical and experimental Otorhinolaryngology. 2010. Vol. 3. No. 4. P. 203-206.
24. Ajalloueyan M. Experience with surgical management of cholesteatomas // Arch otolaryngol head neck surg. 2006. Vol. 132.P. 931-933.
25. Felek S. et al. The functional and anatomical results of the canal wall down tympanoplasty in extensive cholesteatoma. 2009 rock; Vol. 129.P. 1388-1394.
26. Stankovic M. Audiologic results of surgery for cholesteatoma: short and longterm follow-up of influential factors // Otology Neurotology. 2008. Vol. 29.P. 933-940.
27. Kos M, Castrillon R, Montandon P, Guyot G-P. Anatomic and functional longterm results of canal wall down mastoidectomy // Ann Otol Rhinol Laryngol. 2004. Vol. 113 (11). R. 872-876.
28. Bercin S. et al. Results of revision mastoidectomy // Acta otolaryngologica. 2009. Vol. 129. P. 138-141.
29. Ayache S., Tramier B., Strunski. Otoendoscopy in cholesteatoma surgery of the middle ear: what benefits can be expected? // Otology and Neurotology. 2008. Vol. 29 (8). R. 1085-1090.
30. Marchioni D., Mattioli F., Alicandri-Ciufelli M., Presutti. Endoscopic approach to tensor fold in patients with attic cholesteatoma // Acta Otol-Laryngologica. 2009. Vol. 129. P. 946-954.
Cholovik, 33 rock. Diagnostics. The last patient had surgery on the right vus (ocular tympanoplasty, chronic otitis media). ENT-lykar wants to cholesteatoma when it is empty and operative. Є Risik of Intraoperative Acceleration, in which case?
Diligence? Yaksho to swear on
Diligence? Yaksho rely on respect for terms of degradation ( Dehiscent jugular bulb), then tse viglyadaє descho іnkshe, but itself: the clear contour of the cross-flow replaces the sigmoid plate. Tsіkavo, scho mav on uvazi Pavlo, little arrow.

I think about food: there may be a cybulin diverticulum, and it can be very close.
Malasia on uvazi degiscenci,
Malasya on uvazi degiscencii, ala rosіyskoyu meowy at once do not know analogies. Sigmoid sinus strenuousness? Diverticulum of jugular cibulin - I don’t think it’s a correct term, it’s better for naked sinus, the same in the context of the Koali closer :)
Degiscency (= prolapse,
Degiscency (= prolapse, vibuhne cybulin from the bottom of the sigmoid plate dilenka) - vrodzhene camp. Pasha is right, in this case there is little destruction of the sigmoid plate, imovirno, cholesteatoma. That is, with visible cholesteatomy, a high rhizic poses a thin line between the facies and veins. Diverticulum of cybulin is a term full of correct, yak on me, if є vibuchne of the cystic contour, zastosovuvati chi ni - on the right of the cutaneous. In this case, in the area of such a diverticulum, destruction has become, more beautifully visible on the Coronal.
Often on skronevikh k_stki you can see the following picture:

є vibuhne cybulin due to the protection of the sigmoid plate, but not true degradation, altogether as a result of the induced vision, є the risk of vena intraoperatively during the destruction of the plate.
Indirect signs of sigmoid sinus relocation There may be: a) malium of the nipple-like growth; b) the lump of the surface of the nipple-like outgrowth; c) close to the growth of the nipple-like-lusky slit to the posterior wall of the ear canal.
I will acquaint atypical position of the dura mater the middle cranial fossa can serve close to the expansion of the supra-nipple crest to the upper cyst of the ear canal and the supra-meatus.
whish danі literary about those who often see the high domes of the cybulin and the great jugular pits, not the small ones (in their practice they were known to be ringing). The temporal jugular fossa is a surgical problem. The large jugular fossa can grow in front and in the middle of the mastoid to the canal of the facial nerve, or occupy all the retro-labial spaces.
The jugular is even wider the hole can reach the bottom the posterior semicircular canal or lie between them and the dura mater. A large jugular fossa can be in contact with the water supply of the anterior and the aperture of the cochlear duct, deforming the duct, modeling its diameter and navigating the anatomical course.
For help X-ray methods You can reliably adjust the width of the jugular opening and the front of the jugular vein cybulin. However, most often the position of the sigmoid sinus can be precisely determined on the operating table, the position of the sigmoid sinus can be seen as the sinus and the cybulin of the jugular vein, as well as the standing of the cybulin in the empty drum.
Measure the cybulin of the jugular veni and the distance to the sigmoid sinus.
Yak visnachiti rosemary tsibulin jugular veni and go from her to the sigmoid sinus, we can see it on empty, de Viconana antromastoidotomy.
From the bottom of the middle cranial fossa along the center of the mastoid emptying to the top of the sprout, the main line is carried out (1). Distance (1) door 35 mm.
per rating to the main axis(1) the same perpendicular choice: line (2) pass through the lower wall of the ear canal; line (3) - from the middle of the fold of the tendon of the digastric omentum; line (4) - from the lower base of the tendon fold of the digastric ointment; line (5) - from the top of the nipple-like outgrowth.
vidrizok(2-5) adjust the distance from the lower wall of the ear canal to the top of the outgrowth and become 20 to 22.5 mm wide. Perpendicular lines, drawn to the main axis, increase the distance (2-5) by three lines.
They put me in the fake, Шо відрізок (2-3) - the distance from the lower wall of the auditory canal to the top of the cybulin of the jugular vein. Interval (2-4) is given to the distance from the lower wall of the ear canal before the cybulin of the vein is presented. Distance (3-4) will show the height of the jugular vein cybulin. Dilyanka (4-5) road from the base of the cybulin to the top of the nipple-like outgrowth. Yak bachimo, in the middle, it turned out to be practically equal and in the middle one up to 7.3 mm (size 6.7 ± 1.2 mm) (div. Fig. 52).
visas the width of the jugular vein cibulin possible by line (4). For the most part, look from the lower base of the tendon fold of the digastric ointment to the main axis (1), as if the width of the cybulin was presented. Our rozrakhunks have a 10 mm door width for the cibulin. The point of overturning the line (4) with the vissyu (1) is placed at the point of the transition of the sigmoid sinus into the cybulin of the jugular vein.
visas tsibulin jugular veni possible by line (4). For the whole width of the cybulin (the distance from the lower base of the fold of the digastric mucosa to the main axis), the distance from the center to the main axis is always perpendicular to the line (3). Perpendicular to the line of the appearance of the cybulin venia.
Dovzhina perpendicular to the line(H), for the height of the cybulin, the distance (3-4). In this rank, the visota of the cibulin becomes 7.3 mm. The point of overflushing of the perpendicular (H) from the line (3) shows the vertex of the cybulin of the jugular vein.
dali viznachaєmo seen between cybulin jugular veniі sinus. For the whole line (3), it is divided into three parts: from the center of the fold of the digastric omentum to the apex of the cybulin (3a), from the apex of the cybulin to the main axis (3b) and from the main axis to the anterior slope of the sigmoid sinus (Sv).
We got rid of Practically equal- 5.5 mm each (5 ± 1.3 mm). Yak bachimo, from the anterior stem of the mastoid emptying to the apex of the cybulin - 5.5 mm, from the apex of the cybulin to the slope of the sigmoid sinus - 11 mm (10 ± 2.2 mm).
With such a rank, distance from the lower wall of the ear canal to the top of the cybulin of the jugular vein, the height of the cybulin itself, and from the direction of the cybulin to the other point of the top of the nipple-like outgrowth, it was flush and in the middle was folded by 7.3 mm.
The mathematical model is presented viconana by us on forty mastoid outgrowths of up to 35 mm. This will be proponently turned to great statistical material. Tse results, recognized by J. Nadol (1991) and A. Asian (1997) at the last thousand piracy in the rim of the basket.
With an increase in the nipple-like appendage of 35 mm, the height of the jugular vein cybulin becomes 8 ± 2 (mm), from the lower stem of the outer auditory meatus to the apex of the cybulin - 9 ± 2 (mm).
With an increase in growth less than 35 mm, the height of the jugular vein cybulin is 5.3 ± 3 (mm), from the lower stage of the outer ear canal to the apex of the cybulin - 6.6 ± 3.5 (mm).
With an increase in the growth of more than 35 mm, the height of the jugular vein cybulin is 6 ± 2.9 (mm), from the lower stem of the ear canal to the apex of the cybulin - 8.5 ± 3.7 (mm).
25.01.2017
When the kam'yanisty part of the curtain brush is presented, the shape is irregular. The anterior surface is similar to an arcuate papuloid, and the posterior surface, which passes into the furrow of the sigmoid sinus, is reduced.
Analysis of the pre-cranial cyst on radiographs in the main and preadopted oblique projections of the cranium.
Scythe projection. The correct placement on the target X-ray in an oblique projection (Fig. 49) controls the visual appearance of the lateral and internal auditory openings to the lateral side.
The projection-shortened part of the kam'yanist begins to appear before the slidzhuvanoi side. In the front and in the lower slope, there is a slope-lower slope slope (44), behind - a nipple-like outgrowth (21).
Pidstava kam'yanist_y part of the curtain brush has an irregular tricyte shape. The anterior surface її (15), is similar to an arcuate pidnose papilla, and the posterior surface, which passes into the sulcus of the sigmoid sinus (20), is reduced.
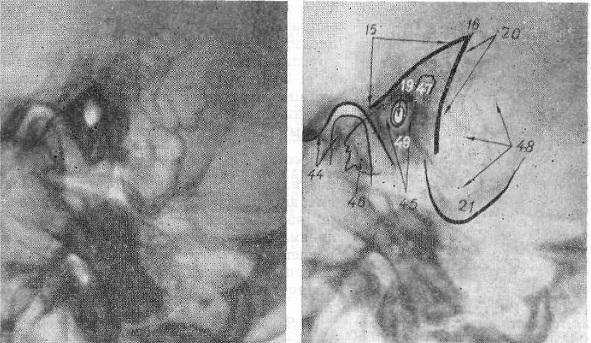
Small. 49. Roentgenogram і a diagram of a skirting brush in oblique projection (according to Schüller). 15 - anterior surface of the rocky part of the curtain brush; 16 - kut Chitelli; 19 - open the call and internal rumors; 20 - furrowed sigmoid sinus; 21 - nipple-like outgrowth; 44 - skrone-lower slit slope; 45 - the "core" of the cyst labyrinth: 46 - the top of the stone part. Povitronosnі midway; 47 - nipple-like stove; 48 - nipple midline; 49 - drum midsection
At the point of transition of the front surface to the rear, there is a gostry kut, which is a projection of the outer edge of the upper edge of the rocky part of the curtain brush (Kut Chitella - 16). The upper part of the rocky part (46) is distinguished from the pracea, as it is projectively built up from the skrone-lower-slit slope.
Ostann_y, yak roztashovus close to the cassette, give a readable image (44). Kindly quilted the head, the hollow and the slope between them (the X-ray anatomy of the skrone-lower slope slope is seen below). The central viddil of the stone part of the early cyst is given an intensive period of time, enriched with a strong cystic speech, which smells out the elements of the inner vuh and removes, as it meant, the vistula, called the “nucleus” of the cyst. When properly placed in central department The "core" of the cyst labyrinth is designed to be a circular form of enlightenment, which represents the total image of the ringing and internal auditory passages (19), as well as drum emptying. Around the "core" of the cyst labyrinth, there is a design of the turn-based rooms, which are located in the upper-back side of the stone-type part of the low-speed chain. Naybіlsha airways lie beside the middle behind the "nucleus" of the cystic labyrinth and is called the nipple-like pyre (47). Back and down to the “nucleus”, the labyrinth grows with a nipple-like growth (21).
Small. 50. X-rays of the stone part of the early brush in the oblique projection (according to Schüller). Variants of pneumatization of the nipple-like appendage:
a - pneumatic; b - partly pneumatic; in -not pneumatized (sclerosed). Single arrows indicate an arc-like movement, sub-lower ones - a drum dah.
Variants of pneumatization of the pancreatic brush can be analyzed most often on the radiograph in oblique projection (Fig. 50). There is a great range of pneumatization of the nipple-like outgrowth and the quickest assessment of the number of types of the nipple-like outgrowth. To characterize the stage of pneumatization of the skrone brush, broken down into different classification schemes. The most widespread in our country was promoted by D.G. Increased pneumatized (a), frequently pneumatized (b) and non-pneumatized (sclerosed), nipple-shaped growths. Vvazhayut, that the steps of pneumatization lie in the form of special features of the development of the nipple-like outgrowth.
Vіkovі specialties. The nipple-like outgrowth is formed internally. At the first time of life, the pneumatization of the drum-like chisel and the nipple-like pyre develop with a slice of mucus shells in them, which covers the drum emptyings. The growth of the mucous membrane expands on the cyst carcasses of the empty sponges of the nipple-like appendage and rests down to the newest appendages of the early fold, which are re-developed in the coma. In the norm up to 5 rocky nipple-like outgrowth is also pneumatic.
Small. 51. Roentgenograms of the stone part of the early brush in oblique projection (according to Schüller).
Variation of the position of the furrow of the sigmoid sinus and cybulin of the jugular vein:
a - sinus relocation; b - lateroposis of the sinus; c - the temple standing of the jugular veni cibulin.
The arrows indicate that there is an external auditory opening and the anterior contour of the furrow of the sigmoid sinus;
However, the development of the pneumatic empty spaces is trivial with the stretching of the life of the people. Winning of the ignition process of the middle vuha in an early child's development of the pneumatization of the nipple-like outgrowth. In this case, in the Danish hour, I will increase the pneumatized outgrowth, which will represent the normal process of developing pneumatization, and often pneumatized and not pneumatized to indicate the destruction of the second. X-ray visualization of the pneumatic structure of the nipple-like outgrowth is of little importance. So, in pneumatic growths, it is gostry perebig ignition processes for the type of valve, and in non-pneumatic - chronic.
On the targeted X-ray of the early brush in oblique projection, the radiologist can make a detailed analysis of the structure, progression, and also pneumatization in the middle of the middle brush on the right and left side. The lack of rosette between the middle partitions and the darkening of the middle part is characteristic of the hot ignition process.
In case of vivchenni variants of the Budovian part of the earliest brush for otolaryngologic clinics, it is important to analyze the anterior (15) and posterior surfaces. Yak denoted a vische, the anterior opucleus contour of the rocky part of the images of the arched peduncle (Fig. 50 b, c; it is indicated by a single arrow), as if projected to be projected to zbіgaєsya behind the contour of the drum dahu. With a significant development of the arcuate underneath, it is not possible to get out of the projection of the drum dahu (designated by single
arrows) і I set up the additional contour, the straightening of the eye and parallel to the contour of the drum dahu (denoted by the sub-line arrow, Fig. 50b). At the norm, the distance between the drum and the upper edge of the ear canal should be 4 5 mm. Viznachennya vіdhilen tsієї vіdstanі from the middle version of the norms of value when the plan of operational engagement is folded.
For the purpose of visualizing the appearance of the sinuous growth of the furrow of the sigmoid sinus and the jugular, it is necessary to analyze the contour of the posterior surface of the stone part of the early cyst. Borotia of the sigmoid sinus can be ribbon-shaped, flat, 8-10 mm wide, spread behind the stone part (div. Fig. 49). The process of enlightenment is clearly visible in the case of a repeated pneumatization of the nipple-like outgrowth. When the pneumatization of the ridge of education is turned, the furrowing of the sigmoid sinus is poured, it is not clearly differentiated on aphids of the nipple midsections.
Directly from the pneumatization of the outgrowth, the posterior surface of the rocky part is clearly contoured; in the last form of the sigmoid sinus є the anterior wall of the furrow of the sigmoid sinus. Gliboka, protruding to the stone part of the sigmoid sigmoid sinus and on the dodatkovy intensive contour.
When a planned operation on the nipple-like outgrowth, it is necessary to clarify the minimum appearance of the empty drum to the anterior groove of the sigmoid sinus. On the roentgenogram of the skylight in the oblique projection of the tympanum, the projection bears the projection of the auditory opening; zazvychay reach 12-14 mm (fig. 51). Increase the size of the sinus to be less than 10 mm (Fig. 51 a). Hirurg is guilty of sinus relocation due to the lack of safety during surgery and the possibility of widening the infection from the middle of the day, to slow down the development of sinus thrombosis.
Less reliable data can be recognized for the additional radiological method of follow-up when the sigmoid sinus groove position is designated as lateroposis (Fig. 51b). From lateral position of the sinus, it means the growth of the furrow in the back wall of the skull. Gliboka furrow on the roentgenogram even more readily ribbon-like education, however, the steps of the furrow, as in the middle variants of the glibine furrow, can be reduced by the summation of the highly pneumatised drum and nipple-like median. In addition, it is important to understand the anatomical and radiological understanding of the later position in the general communication. Clinification of sinus lateroposis may have two options on uvaz: first, if it is borne to produce a significant vitality of the brush along the bottom of the furrow, other, if the flat of the other boron is removed on the trades. In case of cich variants, with aphids, the first to be looked at by anatomists and radiologists like lateroposis, it is not safe to cut through the bottom of the sinus furrow during the operation of the same. This is an insult to the significant options in otolaryngology to develop as a lateroposis of the sinus.
Small. 52. Sketch of the milling of the cutter of the rim brush (a). Roentgenogram (b) і diagram (c) of the pre-brush in transverse projection (according to Stenvers).
19 - callous rumors of the passage; 21 - nipple-like outgrowth; 23 - upper edge of the rocky part of the curtain brush; 24 - opening the і canal of the internal auditory canal; 24a - facial nerve; 24b - vestibular ultkovy nerve: 37 - kamyany-potylic synchondrosis; 45 - "core" of the cystic labyrinth; 46 - top of the rocky part of the curtain brush; 47 - nipple-like stove; 54 - Drum empty auditory brush; 55 - drum dakh; 56 - arc-like pidnesennya; 57 - three-part impression; 58 - semi-circular channels; 58a - anterior;, 58b-lateral; 59 - rablik; 60 - sleepy canal; 60а - vertical part of the carotid canal; 61 - auditory tube. The canal of the facial nerve of meanings by dashed lines, before the day is designated by the star.
On the target X-ray of the early brush in the oblique projection, the canal of the nipple-like veni-vipusnik does not appear early (Fig. 51 a; meanings of the small arrow), but there is little visibility with clear, intense contours. The internal openings to the canal of the nipple-like veni-vipusnik begin to appear in the middle third furrow of the sigmoid sinus. It is possible and larger in the upper part of the inner opening on the cordon from the groove of the transverse sinus. It is necessary to carry out the operation during planned operations, as the canal of the nipple-like veni-viper can be
have a meal in the operative field, in conjunction with which you might get hurt.
The name of the nipple-like opening to the canal of the nipple-like veni-vipusnik, which appears at the side of the nipple-like outgrowth, or in the area of the papillary-nipple-like suture, appears less readily on the x-ray images.
On the targeted radiographs of the early cyst in oblique projection, with a high standing of the cybulin of the jugular vein, the jugular pit, in the yaky vona zalyagє, should appear at the vigilance of the education with a clear projection of the upper contour, rosy The high standing of the cybulin of the jugular veni is treated with surgery during planned operations.
In the same projection, there is a skrone-lower slit slope.
Transverse projection. On the sighting X-ray of the skirting brush in the transverse projection (Fig. 52b) of the Kamyanist, the part is shown to be intensively uneven and visible on all protrusions from the top to the base without projections. On the upper edge of the rocky part of the curtain cistern (23), there is a quilt: the base is solidified, shaped like a drum (55), medially - arched underneath (56), at the top - threefold depression (57). From the drum, the middle of the stone part of the drum can be seen, and even lower, when entering the edge-forming viddil, the nipple-like protuberance from the air cells grows along the side of the lane (21). From the arcuate underneath, the "core" of the cystic labyrinth clearly begins (45), on the smallest way, there is a line of enlightenment of the two canals (58): the front (vertical) and the lateral side (horizontal) Medially and from the bottom to the front є the education of the spinal canal (59), and medially and from the side of the straight ribbon-like education of the internal auditory canal (24), which is beyond the reach of the top of the rocky part. In the area of the upper, lower than the internal auditory canal, there is a smaller opening, a little more wider education of the carotid canal (60), and even lower - the higher one, a ribbon-like education of the stony-papillary sinchondrosis is clearly oxidized (37).
The slope-lower slope slope, the projecting of the lower rocky part in front of the nipple-like outgrowth, is meaningfully projected because it is not due to X-ray anatomy.

Small. 53. Roentgenogram і a diagram of a skrone brush in an axial projection (according to Mayor). 15 - anterior contour of the stone part of the early brush; th - back contour of the rocky part of the skinny brush; 24 - internal auditory passage; 46 - top of the Kamyanist part; 47 - nipple-like stove; 54 - the image of the outer ear canal and the empty drum with the auditory beads; po - sleepy channel.
Axis projection. On the target X-ray of the early brush in the axial projection (Fig. 53), the correctness of the arrangement is reconverted according to the projected image of the empty drum from the earliest auditory passage to the lateral side. The Kamyanian part is meaningfully projected, and yes, it is intensively uneven with clear contours between the middle and posterior fossae of the skull (15, 20). In the region of the posterior fossa of the skull, there is a lambda, thyme-nipple-like and pill-nipple-like suture. In the area of the base of the stone part to the posterior contour, there is a ribbon-like enlightenment, a furrowed sigmoid sinus.
At the beginning of the rocky part, projectionally, there is a rotational nipple-like midsection, in front of which there is a greater wrong form of education, like a nipple-like pyre (47).
To the bottom and in front of the nipple-like pyre, on the level of the “nucleus” of the cystic labyrinth, the differentiation is not uniformly enlightened by the oval of the new form with clear contours, which is a total image of the ear drum
In the area of the upper part of the rocky part, closer to the front contour, there is a quilted form of clear enlightenment, surrounded by a sleepy canal (60). Above it, closer to the posterior contour, an analogous enlightenment begins to appear in the visualization of the internal auditory canal (24). A bit in front of the upper part of the rocky part of the curtain brush is projected to increase the slope-lower slope slope.
Tags: x-ray, skroneva kistka, analysis, pneumatization options, vikov zmini, kam'yanista chastin
Ear of activity (date): 01/25/2017 9:54:00
Kim Folds (ID): 645
Key words: x-ray, skroneva brush, analysis, pneumatization options, vіkovі zmіni



